
Medicare Lead Generation for Agents: The Complete Guide
Why Most Medicare Agents Struggle With Lead Generation
The traditional approach goes like this: buy leads from a vendor, call them as fast as possible, hope you get there before the other agents who bought the same list.
That model worked fifteen years ago. It doesn't work now.
Here's why.
The Medicare market has gotten more competitive, not less. 10,000 people turn 65 every day in the United States. That's real demand. But the lead vendors know it too. They sell the same prospect to three, four, sometimes five agents. Everyone races to the phone. The prospect gets five calls in an hour and stops answering.
The result: low contact rates, low booking rates, burned money.
Most agents blame themselves. They think they need a better script, more calls, or a harder close. But the problem isn't on their end. The problem is the lead.
When you start with a bad lead, no script can fix it.
The Shared Lead Trap
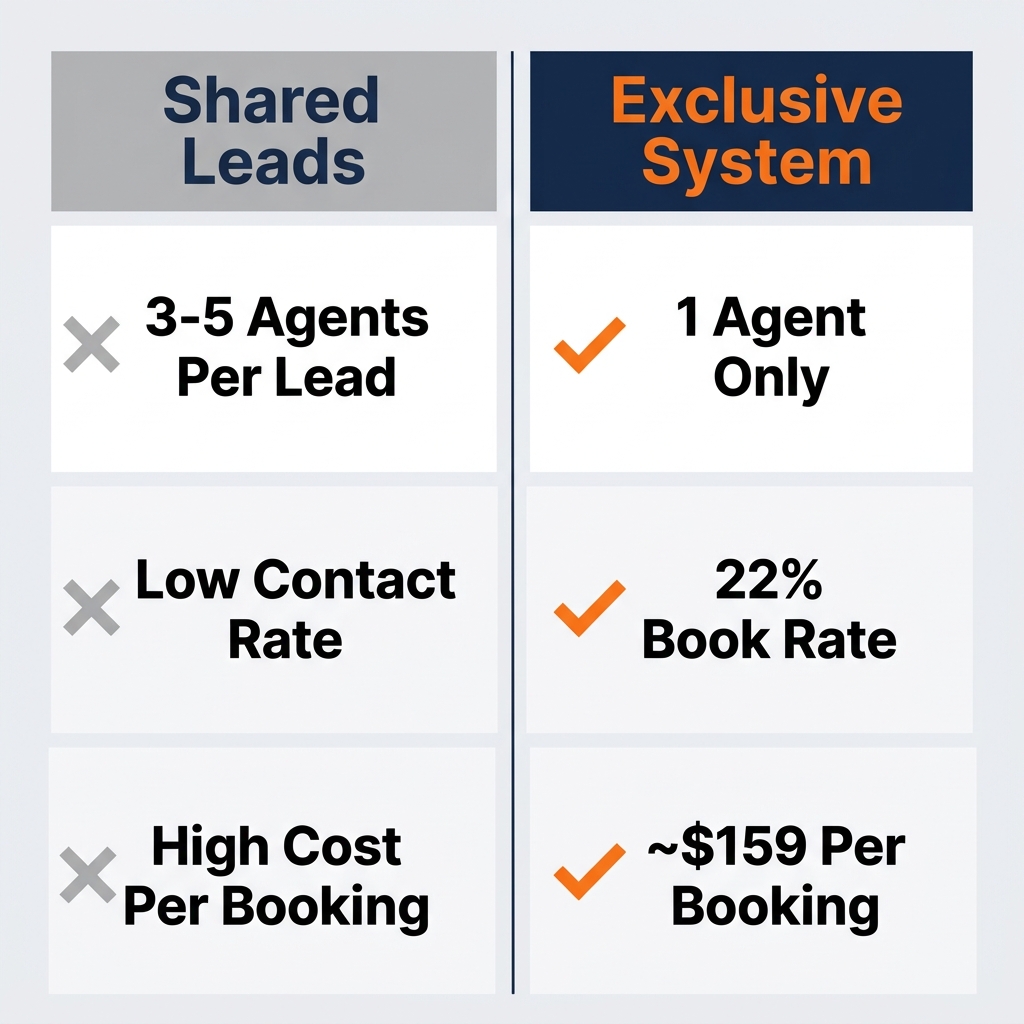
Shared leads are exactly what they sound like. One prospect fills out a form — maybe they clicked an ad, maybe they answered a survey — and that record gets sold to multiple agents simultaneously.
The vendor makes more money selling it four times than once. The prospect gets overwhelmed. The agent loses.
Here's what the math looks like in practice.
A shared Medicare lead might cost $15–$25. Sounds cheaper than an exclusive lead at $35–$50. But cheap per-lead cost doesn't mean cheap per-appointment.
If you're calling leads that five other agents already dialed, your contact rate drops. Your booking rate drops. You work more to get the same result — and you pay more per actual appointment than the agent who bought exclusive leads and skipped the race.
This is what we call the real cost of a Medicare lead. It's not the sticker price. It's what you actually pay per booked appointment after contact rate and booking rate are factored in.
We wrote a full breakdown of this math here: The Real Cost of a Medicare Lead →
What a High-Quality Medicare Lead Actually Looks Like
Not all leads are created equal. Here's what separates a good Medicare lead from a bad one.
Exclusive. The lead was generated for you and only you. No other agent is calling the same person at the same time.
Real-time. The prospect just raised their hand — minutes ago, not days. Contact rates drop sharply as time passes. A lead that's 72 hours old is a fraction as valuable as a fresh one.
Intent-qualified. The prospect answered specific questions about their situation. They're not just someone who clicked a banner ad. They expressed genuine interest in Medicare coverage.
T65-targeted. A T65 lead is someone turning 65 — entering their Initial Enrollment Period (IEP) for the first time. They've never been through Medicare enrollment before. They're open to guidance. They have a deadline (their birthday month) that creates natural urgency.
These four qualities together define what a real Medicare appointment opportunity looks like. Any lead source you evaluate should be measured against them.
The 4 Best Channels for Medicare Lead Generation
There is no single channel that works for everyone. But these four produce consistent, scalable results for independent Medicare agents.
1. Meta Ads (Facebook + Instagram)
Meta ads are the most scalable channel for Medicare lead generation right now.
Here's why. Facebook and Instagram have massive user bases in the 60–70 age range. That's your Medicare market. You can run lead generation campaigns that capture prospect information directly inside the platform — no website required.
The targeting works differently than it used to. Meta's Special Ad Category rules for insurance restrict certain demographic filters. But the platform's algorithm compensates. When you run a well-structured campaign with a clear offer and strong creative, the algorithm finds your audience.
A well-run Meta campaign for Medicare agents targets T65 prospects — people turning 65 within a defined window — using interest-based and behavioral signals. The lead flows into your CRM in real time. An automated follow-up sequence starts immediately. Your setter calls within minutes.
At target performance, expect around $35 per lead. That's not guaranteed on day one — the algorithm needs 10–14 days to learn. But it's a realistic steady-state CPL for a campaign running properly.
The key variable is what happens after the lead comes in. Meta gets you the prospect. Your system — your follow-up speed, your CRM automations, your setter — determines whether they book an appointment.
More on this in a minute.
2. T65 Targeting
T65 targeting is the most consistent year-round lead source available to Medicare agents.
Ten thousand people turn 65 every day. Unlike AEP, which concentrates demand into a 53-day window where every agent is fighting over the same pool, T65 leads are available every single month of the year.
The IEP — Initial Enrollment Period — runs for 7 months: 3 months before the 65th birthday through 3 months after. That's your window. The prospect has a real deadline and a real reason to make a decision now.
T65 prospects also tend to be more receptive. This is their first time enrolling in Medicare. They don't have a plan they're attached to. They're not comparing your pitch to the last three agents they talked to. They're learning the system for the first time — and they want help.
We wrote a detailed breakdown of T65 targeting here: T65 Facebook Targeting for Medicare →
3. Organic Search (SEO)
SEO is the slowest channel to start, but the cheapest per lead once it's working.
When a Medicare agent in your market types "how to get Medicare coverage turning 65" into Google and finds your blog, that lead cost you almost nothing. No ad spend. No vendor fee. Just the time and effort of creating useful content.
The limitation: SEO takes 6–12 months to gain traction. It's not a lead source for next month. It's an investment in 2027 and beyond.
For independent agents with limited budgets, a simple content strategy — answering the questions your prospects are actually Googling — can build a meaningful inbound pipeline over time.
For agencies running paid ads, SEO complements it. Paid ads get you appointments now. SEO reduces your dependency on paid traffic over the long run.
4. Referral Partnerships
Referrals from existing clients and professional partners (elder law attorneys, financial advisors, hospital discharge planners) are high-conversion leads with zero acquisition cost.
The downside: referrals don't scale predictably. You can't decide to run 50 referral leads next month the way you can scale a Meta campaign. And most agents who rely primarily on referrals are one or two key relationships away from a dry pipeline.
Referrals should be part of your mix — not the whole strategy.
The Full System: From Lead to Booked Appointment
Getting a lead is only step one.
Most agents lose money not because they can't generate leads, but because their system after the lead is broken.
Here's what a working Medicare lead gen system looks like end to end.
Step 1: Lead comes in. The prospect fills out a form from your Meta ad. Their information routes into your CRM — GoHighLevel is the tool most Medicare agencies use for this.
Step 2: Immediate automated outreach. Within 60 seconds, an automated SMS and email go out. The message is warm, not salesy. It confirms you received their info and sets the expectation that someone will call.
Step 3: Setter calls within minutes. A setter — either you or a dedicated team member — dials within the first few minutes. Speed to contact is the single biggest variable in booking rate. The faster you call, the higher your contact rate.
Step 4: Appointment booked on the calendar. The setter's job isn't to sell. It's to confirm the appointment. They qualify the prospect, answer basic questions, and book a specific time on your GHL calendar.
Step 5: Pre-appointment confirmation sequence. Automated reminders go out 24 hours before and 1 hour before. A setter calls to confirm. This drives show rate.
Step 6: The appointment. You run the call. Your job starts here.
We covered the full GHL setup for this system here: GHL for Medicare Agents →
The system sounds simple. But most agents are missing two or three steps. Each missing step costs show rate, booking rate, and enrolled clients.
The Real Math on Medicare Lead Generation
This is where most lead discussions go wrong. Agents compare CPL and stop there.
The number that actually matters is cost per enrolled client.
Here's how to calculate it using real benchmarks.
Start with your CPL. At target: ~$35 per lead.
Apply your book rate. Industry benchmark for a well-run system: 22%.
That means roughly 1 in 5 leads books an appointment.
Cost per booked appointment: $35 ÷ 22% = ~$159
Apply your show rate. Benchmark: 75%.
Cost per showed appointment: $159 ÷ 75% = ~$212
Apply your close rate. Benchmark: 30%.
Cost per enrolled client: $212 ÷ 30% = ~$707
Now compare that to what a Medicare Advantage client is worth.
Year 1 MA commission: $611. Your cost to acquire: $707. You're slightly underwater in year 1.
But Year 2 renewal: $306. By renewal, your cost to acquire is fully covered and the client is pure margin.
Five-year LTV of one MA client: $1,500–$2,000.
Every $707 you spend to enroll a client returns $1,500–$2,000 over five years if they stay on the same plan. That's the investment case for a real lead gen system — not just the first year.
And that's before cross-selling. An MA client who stays with you has real potential for Final Expense, life insurance, and annuity conversations over time. The full cross-sell path can multiply the LTV of each enrolled client significantly.
We broke down the LTV math in detail here: Medicare Advantage Client Lifetime Value →
How to Evaluate Any Medicare Lead Source
Before you spend money with any lead vendor, channel, or agency, run it through these five questions.
1. Are these leads exclusive? If the same lead is going to other agents, your effective CPL is higher than it looks. Ask directly: how many agents receive this lead?
2. How fresh are they? Real-time leads close at a dramatically higher rate than aged leads. Ask about the average time between form fill and delivery.
3. What's the actual contact rate? Not the number the vendor quotes. Your real contact rate with real calling effort. Test with a small batch before committing to volume.
4. What targeting was used? T65-targeted leads outperform broad Medicare leads. Ask what the age targeting was and how the prospect was qualified.
5. What's your cost per booked appointment — not cost per lead? Run the math above. CPL is a headline number. Cost per booked appointment is the number that matters for your business.
A lead source that looks expensive per lead can outperform a cheap one by 3x when you factor in contact rate and booking rate. This is exactly why shared leads often cost more than exclusive leads when you do the real math.
Building a Year-Round Medicare Pipeline
Sixty to seventy percent of Medicare lead volume concentrates in AEP — the 53-day window from October 15 to December 7.
Most agents feel this in February. AEP ends. Referrals slow. The leads they bought cost more because everyone else is buying too. Income gets lumpy.
The answer isn't to work harder in AEP. It's to build a pipeline that runs the other 10 months.
The IEP is the most underused opportunity in Medicare sales. Every month of the year, a wave of people hit their 65th birthday. They have a 7-month window to enroll — 3 months before and 3 months after their birthday. They're available now, not just in October.
Agents who target IEP prospects consistently report steadier income and less competition. AEP is a fight. IEP is a conversation.
A T65-focused Meta campaign, running year-round at a sustainable budget, creates the pipeline that most agents say they want but few actually build.
We covered how to build it here: How to Build a Year-Round Medicare Pipeline →
The Difference Between a Lead Vendor and a Lead System
Most lead vendors give you data. A name, a phone number, and a form fill.
What happens next is your problem.
A lead system is different. It generates the lead, routes it instantly, triggers follow-up automatically, books the appointment, sends reminders, and handles no-shows with a recovery sequence. Every step is designed and tested.
The difference in output — booked appointments, show rate, enrolled clients — is significant.
An agent buying shared vendor leads and calling them manually is competing on hustle. An agent running a system is competing on infrastructure.
Most independent agents underestimate how much the system matters. The best lead in the world doesn't book itself.
What a Real Medicare Lead Gen Budget Looks Like
For a solo agent or small team, here's a realistic monthly structure for a Meta-based T65 campaign.
Ad spend: $1,000–$1,500/month At $35 CPL, that generates roughly 28–43 leads per month.
Expected bookings at 22% book rate: 6–9 appointments
Expected shows at 75% show rate: 5–7 appointments
Expected enrollments at 30% close rate: 1–2 clients
Year 1 revenue from 2 MA enrollments: ~$1,222. Year 2 renewals (same clients): ~$612. Five-year cumulative from those 2 clients: ~$3,000–$4,000.
That's from one month of lead gen spend. Compounded over 12 months — with consistent volume and a system that actually works — the math changes substantially.
This doesn't account for cross-sells, referrals from enrolled clients, or the cumulative effect of a growing book of business.
What to Do Next
Medicare lead generation isn't complicated. But it does require a system — not just a lead source.
The agents writing consistent appointments in January, March, and July aren't doing anything magical. They built the infrastructure. Exclusive leads. Real-time routing. Automated follow-up. Setter coverage. Pre-appointment confirmation. A CRM that handles it all.
Most agents know what the system should look like. The gap is in building it, testing it, and running it consistently.
Want to know exactly where your current lead gen setup is breaking down?
Take the free 60-second assessment and get your personalized Medicare Lead Gen Roadmap. It benchmarks your pipeline against what a working system looks like and shows you exactly what to fix first — free, no pitch.
[Get Your Free Medicare Lead Gen Roadmap → https://sixtyfive-leads.lovable.app/roadmap]
Frequently Asked Questions
Q: What is the best way to get Medicare leads as an independent agent? A: The most scalable approach is a Meta ads campaign targeting T65 prospects — people turning 65 — with exclusive, real-time leads routed into a CRM like GoHighLevel. This creates a year-round pipeline that doesn't depend on AEP, referrals, or shared lead vendors. The system matters as much as the lead source — booking rate and show rate are determined by what happens after the lead comes in.
Q: How much does it cost to generate a Medicare lead? A: Target CPL for a well-run Meta campaign is around $35 per lead. But cost per lead is the wrong number to optimize. What matters is cost per booked appointment (~$159 at 22% book rate), cost per showed appointment (~$212 at 75% show rate), and cost per enrolled client (~$707 at 30% close rate). A cheap lead with a low contact rate will cost more per enrolled client than a slightly more expensive exclusive lead.
Q: What is the difference between exclusive and shared Medicare leads? A: Exclusive leads are generated for one agent only — no other agent receives the same prospect. Shared leads are sold to 3–5 agents simultaneously, creating a race to the phone that drives contact rates and booking rates down. Exclusive leads cost more per lead but typically cost less per booked appointment when you factor in actual contact and booking performance.
Q: How do you build a year-round Medicare pipeline instead of just AEP income? A: Target IEP prospects — people turning 65 — instead of relying on the AEP enrollment surge. The IEP runs 7 months (3 months before to 3 months after the 65th birthday), every month of the year. Running a consistent T65 Meta campaign with year-round budget creates steady appointment volume in every month, not just October through December. Agents who do this report significantly more consistent income and less competition on each call.
